

 If you’re a comprehensive ophthalmologist, this year feels like every year as patients filled waiting rooms and appointment calendars overflow. If you’re an elective vision specialist, you’re grateful for cataract surgery, where patients still need lenses removed and are open to Lifestyle IOL discussions. If you’re a LASIK surgeon, you’re wondering where the market went. Phones are quiet. Appointment calendars show gaps. Employees are hovering in kitchens and break rooms. And industry experts paint a continued bleak picture.
If you’re a comprehensive ophthalmologist, this year feels like every year as patients filled waiting rooms and appointment calendars overflow. If you’re an elective vision specialist, you’re grateful for cataract surgery, where patients still need lenses removed and are open to Lifestyle IOL discussions. If you’re a LASIK surgeon, you’re wondering where the market went. Phones are quiet. Appointment calendars show gaps. Employees are hovering in kitchens and break rooms. And industry experts paint a continued bleak picture.
In the midst of this uncertainty, practice inboxes and mailboxes are filling up with marketing and practice development offers. Webinars. Seminars. Boot camps. Practice coaching. The most prominent messages in this cacophony are: “Keep marketing spending high,” “Make LASIK affordable” and “Address the fear.” Yet, if we parse the financial data from LCA-Vision and AMO, we can derive very clear results for the strategic and executional issues we each question in marketing LASIK today. In this article, we will look at what the market — our prospective patients — have said, as demonstrated by public financial data.
In the practices we advise, we made a decision that LASIK is facing a fundamental reset as baby boomers age out of the LASIK market, and Millennials haven’t embraced LASIK as a necessary option. So what should you do? Spend within your means. More than ever, you must know the intricacies of profitability benchmarks and adhere to a plan that is sustainable over the long term. Here are three financial markers that you should meet or beat to thrive long-term in LASIK practice.
■ Total marketing spending: It should be no more than 15% of gross revenue. Once you are established and delivering great results this can drop closer to 10%, but your expenditures will always be high compared to non-elective practices because you are in a constant state of generating new prospects.
■ Cost per surgery (CPS): It should be no more than 15% of the average collected global fee. So for the industry average of $2,000/eye, CPS should be $300. At 100 eyes per month, your marketing budget should be $30,000. Collected revenue should be $200,000 monthly.
■ Cost per lead (CPL): Cost per lead and cost per surgery should be almost identical if your practice converts patients effectively. For every 10 people that inquire, 75% should attend a consultation. 75% of those people should convert to surgery. Averaging in monocular and binocular treatments, you should expect each person to equal 1.8 eyes. Therefore, 10 x 75% x 75% x 1.8 = 10. This formula is easy to remember because, if conversion is in balance, 1 inquiry should equal 1 surgical eye.
Does spending above these benchmarks in today’s LASIK climate work? No practice can make money with more than 20% of revenue spent on marketing. Don’t spend beyond profitability. The market simply isn’t reacting to increased spending.
Every LASIK practice knows its advertising must address one of two core issues: Fear and Finances. Prior to the 2008 recession, our focus on financing drove a great deal of profitable LASIK activity. But similar to the entire economy drunk on credit, the financing offers for LASIK continued to ratchet up. Payment plans gave way to “interest-free.” One-year programs extended to 18 and 24 months. And interest-free became no interest and no payments. At every escalation, this program became more and more expensive to the practice. Financing costs should be considered a marketing expense and calculated in cost per surgery, because the more lenient financing plans can now significantly eat into collected LASIK fee.
What was once a great LASIK selling feature might be, in some instances, becoming a liability.
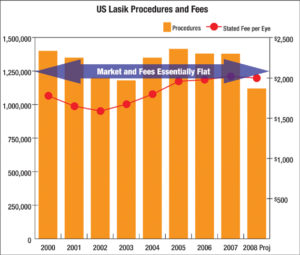
Historical U.S. LASIK procedure volume & fees.
I believe there is one single best way for us to grow the LASIK market, and it’s the elephant in the room that often gets overlooked. Deliver 20/20 vision 100% of the time. Or rather, 20/Happy, which is patient-preferred vision, 100% of the time. That might be 20/20 distance or 20/Happy Monovision, or -1 D bilaterally for the 48-year-old woman who spends most of her day at a computer. It’s that simple, and that complicated. Before you begin discounting all the reasons you can’t deliver 100% vision satisfaction, let’s step back and examine the history of how we have dealt with patient fear.
First, we all agree that no one volunteers to have their eyes touched. No one wants to have eye surgery. But they do, when the disability and frustration and inconvenience of glasses or contacts propel them past fear into action. And how have we encouraged them to trust us with their eyes? We started with surgeon experience: “I’ve done more than him.” But when the difference between his 2,000 and my 10,000 procedures became non-motivating, we went to technology. “Mine is better than hers.” And better over the years has meant expanding from myopia to hyperopia, from no astigmatism to lots of astigmatism, from surface to flapped, from traditional to custom, from bladed to bladeless. But this ratcheting up of technology, like the ratcheting up of credit terms, hasn’t grown our market one bit. All the technological innovation we’ve enjoyed since 1995 has garnered a market that peaked at 1.4 million procedures and a price point flat of$2,000/eye. Our current market size is 1/2 that peak, and prices are beginning to fall.
Let’s look at how the other large elective surgery specialty — cosmetic surgeons — promote their practices. Do they share results? Absolutely. All the time, at every consultation, you will see “before-and-after” examples of noses and necks and breasts and tummies. You couldn’t be a successful cosmetic surgeon without showing prospects the results of your work. Cosmetic surgeons say they are experienced, and they occasionally mention technologies or techniques that allow them to deliver results, but mostly they promote results — the actual proof of what they deliver.
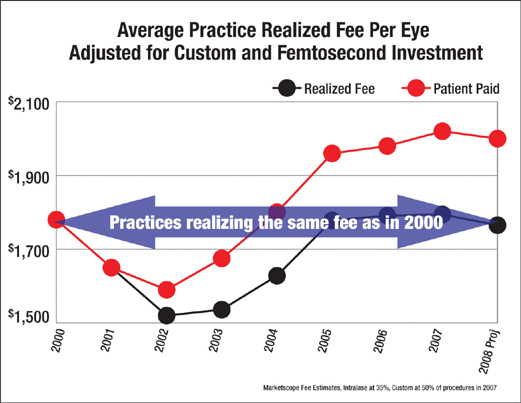
Technology increases patient fees but not practice profitability.
Now compare that to LASIK surgeons. What do we sell? Improved vision. Permanent vision. Glasses-free vision. How do most practices demonstrate results? By talking about surgeon experience or laser technologies. Yet those are the means by which you deliver results. They are not results. This is why we have never created the momentum and acceleration that LASIK should enjoy.
The ultimate patient fear is, “Could this procedure ruin my vision?” And because we as an industry won’t answer that question, we can’t grow. The answer is, “Here are my exact results for every person walking around town with the vision I’ve given them.” The answer is a specific handout that shows your results, on your laser, with your patients, so the prospect sitting in the consultation lounge can clearly see that LASIK is safe, effective and life-changing. Do cosmetic surgeons have informed consents that tell patients what could go wrong? Of course. Do they notshow pictures of representative results simply because one might not turn out perfect? Of course not. Yet we continue to insist that we can’t show patients our actual outcomes because that would be promising something we might not deliver.
In my consulting experience, the reason practices don’t show outcomes to prospective patients is because they don’t know them. They don’t track and record acuities and postop refractions for every eye every visit. They don’t have a living, breathing nomogram that allows them to tighten surgical plans to +/- 0.25 D consistently. Yet these practices believe they deliver great results. I have yet to perform an evaluation of outcomes at the practice level where the results were as good as the surgeon thought they were. This is why we are not growing.
LASIK is good, but it’s not great. The technology available to us with newest-generation lasers yields extraordinary results. But these results are slightly different in every pair of surgeon hands. Practices must invest time, money and employee effort in capturing results, improving outcomes and incorporating that message into LASIK consultations. The answer to LASIK fear is not experience or technology. It’s results. The market tells us that every single day.
So what am I advising our practices do with LASIK in the current environment? Commit to a marketing budget within the 15% guideline. Ensure conversions are strong so cost per lead and cost per surgery are almost identical, and fix what’s wrong if they’re not. Use outcomes to attract new patients. Let people know how great LASIK is. Our practices that use outcomes effectively in marketing are growing — even in this economic climate.
We offer vision. We promise vision. We deliver vision. That’s our strategy — and we are sticking to it.