

 For a practice interested in increasing the number of upgraded IOL surgeries performed, a significant barrier is the appointment calendar. Even suggesting that we modify who we see, or how we see them, may throw staff and physicians into a state of chaos.
For a practice interested in increasing the number of upgraded IOL surgeries performed, a significant barrier is the appointment calendar. Even suggesting that we modify who we see, or how we see them, may throw staff and physicians into a state of chaos.
Both decisions are important for the surgical practice. This article will explain Silo Scheduling, and this article will discuss Block Scheduling in further detail.
Remember the Tony Robbins quote, “If you do what you’ve always done, you’ll get what you’ve always gotten.” For most comprehensive ophthalmologists, the practice you have is predicated on who calls. Should caller demand be the deciding factor in the patient mix of your practice over the next 20 years? Enter Silo Scheduling, which is a tool to help you answer, “What types of patients do I want to see?” Silo Scheduling helps you prioritize:
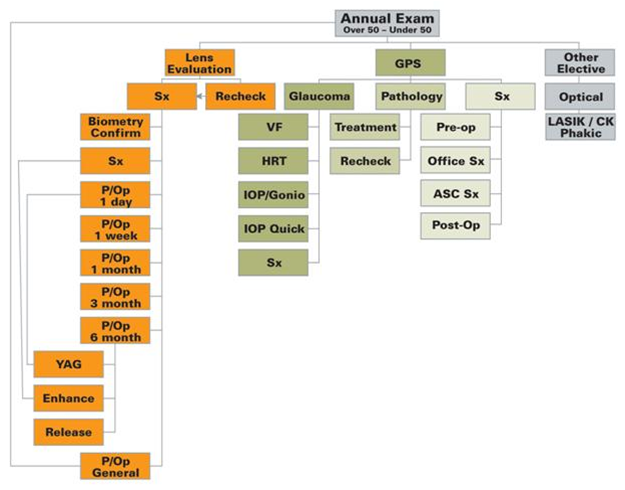 Silo Scheduling defines the broad service lines where you wish to participate. Silos require you to set Visit Type definitions, a process which insures the correct patients will be scheduled in the correct appointments, and education is appropriately at each stage. Silos help you understand which visit types should be restricted or eliminated so they don’t overwhelm the appointment calendar. One example of Silos is shown at right.
Silo Scheduling defines the broad service lines where you wish to participate. Silos require you to set Visit Type definitions, a process which insures the correct patients will be scheduled in the correct appointments, and education is appropriately at each stage. Silos help you understand which visit types should be restricted or eliminated so they don’t overwhelm the appointment calendar. One example of Silos is shown at right.
Once you’ve defined the right Silo structure for your practice, and the percentage you want each silo to represent of your time, you must confirm that the revenue changes which result are positive. Visit Types don’t correlate directly with Diagnosis Codes, so it’s always a bit nerve-wracking to say, “I don’t want to see any more glaucoma,” without a clear understanding of what that means to your bottom line.
To make sure appointment changes create positive financial changes, correlate visit types to diagnosis codes and revenue, as there is not a one-to-one relationship. For every additional Lens Surgery slot we add, we must add an evaluation visit, a biometry confirmation visit, and several post-op visits. Some visits are paid, others are not, so we want to make sure we add the complete package of visits to the calendar that will help achieve more surgery. We also must delete visit types and groupings that we want to see less of, which have a completely different set of financial parameters. What we’ve done at Elective Med is develop an Appointment Mix Summary by Silo correlating diagnosis codes to silos. A practice can then evaluate questions such as, “If I reduce the glaucoma and pathology portions of my practice, and concentrate on growing Lens and LASIK surgery, how will my bottom line be affected?” Performing this Appointment Mix Analysis provides confirmation that changing the appointment template will yield positive bottom line results.
Contact us if you’d like to learn more about Silo Scheduling, establishing a new appointment template, or the financial analysis associated with changing your template.